|
Hypermobility
of the coccyx -1
Jean-Yves Maigne, MD
|
Hyper mobility of
the coccyx is sometimes an easy diagnosis based on the sole radiogram, when the
mobility exceeds clearly 30° in flexion (mobility in hyperextension is very
rare, as we will see in another section), sometimes a more difficult one when
borderline figures are encountered (between 25 and 30° for instance). In these
latter cases, two other radiologic signs can help: a narrowing of the anterior
aspect of the joint with a contact (friction) of the bone surfaces in the
sitting position, and a misalignment of the two involved bones appearing in the
same (sitting) position. These abnormalities (as compared to a control group)
are significant only if the joint is tender at palpation (the involved joint,
and not the joint above or below), and if the injection of either lidocaine or
steroid is successful (at least 2 months for this latter). This means that the
clinical examination has sometimes to be done under fluoroscopic control.
| |
|
Six cases of hypermobility
|
| |
|
|
|
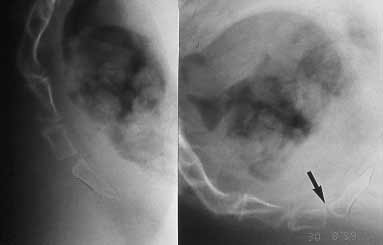
Case #1. This is a typical hyper mobility. The affected joint
is the lower one (arrow), with a flexion of 35°.There is a narrowing of
the anterior aspect of the joint, but without friction of the two bones.
Tiny calcifications can be observed, without specific value. The other
joints are not mobile. |
|
|
|
Case #2. Another case with typical hyper mobility of the first
mobile joint, with 60° of flexion. In the sitting position, there is a
friction between the two bones, which is a supplementary source of pain. |
|
|
|
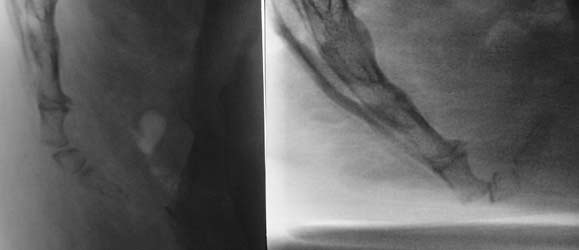
Case #3. A third case. Note that there is no mobility in the
sacro-coccygeal joint. This joint is in no way a source of pain (and is
not tender at palpation, and an injection of steroid at this level would
bring no relief), despite the presence of osteophytes. |
|
|
|
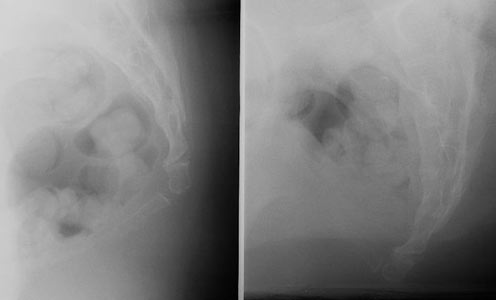
Case #4. No problem here, with a clear diagnosis: flexion>30°,
contact and densification of the bones. To ensure the responsibility of
this abnormality of motion, the joint has to be tender at palpation, and
the injection to be successful at last 2 or 3 months. |
|
|
|
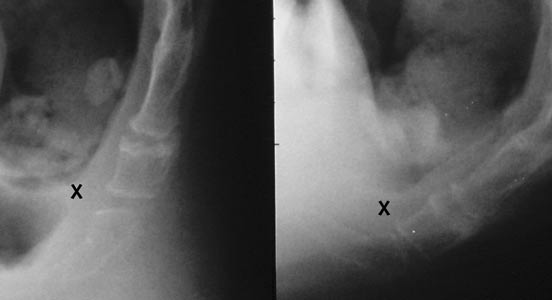
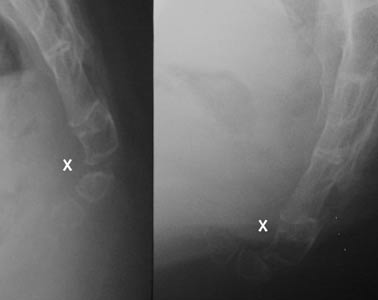
Case #5. The mobility is here around 30°. There is a narrowing
of the joint space at its anterior aspect (X), but without friction.
Note the
irregular aspect of the sacrococcygeal joint, but without any motion,
thus not a painful abnormality. |
|
|
|
Case
#6. This case is borderline. The mobility is just exceeding
25°, but the first mobile bone is eroded at its anterior part by the tip
of the sacrum (X). Furthermore, the joint space was tender at palpation
under fluoroscopic control, and the steroid injection was successful,
establishing the responsibility of the joint. |
|
Comment réaliser et lire les radiographies dynamiques
1 |
|
Luxations
postérieures 1 -
2 |
|
Hypermobilité
1 -
2 |
| Epines
1 -
2 -
3 |
|
Luxations antérieures 1 |
|
Radiographies "normales" |
| Lésions
complexes 1 |
|
Fractures
1 |
|
Calcifications
1 -
2 |
|
Déformations
1 |
|
Anatomie du coccyx |
|