www.sofmmoo.org
Dorsal Thoracic Pain
in Manual Medicine
Jean-Yves Maigne, MD, Physical Medicine, Hotel-Dieu
Hospital, 75181 Paris Cedex 04, France
|
Written 2002.
This article has also been published (text only) in the Journal of Orthopaedic
Medicine (last issue, 2002) with co-author Richard Ellis.
Content of the page:
Nerve entrapment
Muscular sprain
Myofascial pain
Pain referred from the lower cervical spine
Thoracic facet syndrome
Discogenic pain
Psychogenic pain
Summary:
Dorsal thoracic pain is very common, but there is a paucity
of literature on this topic. We present a review of the available literature
on the causes of this syndrome. Cyriax attributed thoracic pain to a disc
protrusion. The mechanism of pain was primarily dural. The clinical features
were the reproduction of the pain under neck flexion contrasting with the
freedom of other neck movements, a limitation in thoracic flexion and an increase
of pain with coughing.
Experimentally,
thoracic discography has partially substanciated this hypothesis. Travell
and Simons describe trigger points in thoracic muscles such as longissimus
dorsalis, iliocostalis, semispinalis, rhomboideus, levator scapula, etc...
The causes for trigger points are many, including trauma, poor postures and
repetitive movements.
Dorsal
thoracic pain is very common, but there is a paucity of literature on this
topic. Different causes have been evoked, such as nerve entrapment, muscular
sprain, trigger points, pain referred from the lower cervical spine, thoracic
facet syndrome, discogenic pain or psychogenic disease. Our aim is to review
theses different sources of pain and to discuss them in light of our own studies
and experience in thoracic pain.
Astvatsaturov
was the first to describe, in 1934, what he called “Notalgia paresthetica”
(notalgia, a Greek name for “pain in the back”). Patients typically
report chronic pain and sensory symptoms that are frequently described as
intense itching in an area 4 to 10 cm in diameter over the thoracic paraspinal
muscles at the inferomedial scapula. There is a diminished pinprick sensitivity
corresponding to an area from T2 to T6 thoracic dermatomes. The injury mechanism
is essentially unknown. Notalgia paresthetica is thought to be caused by a
lesion of a thoracic dorsal primary rami T2 trough T6 (entrapment neuropathy)
which run a long course up through the thick paraspinal muscles. The nerves
appear to be vulnerable to damage as they pursue a right angle course close
to the tip of the spinous process, thus predisposing them to harm from otherwise
innocuous insults of a varied nature. Investigations are not helpful in confirming
the pathogenesis.
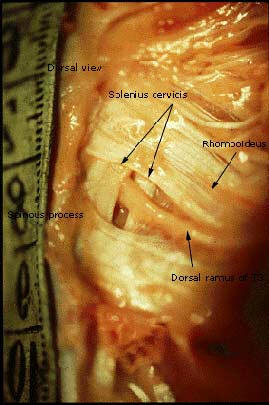
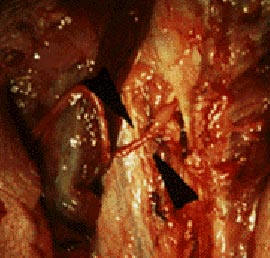
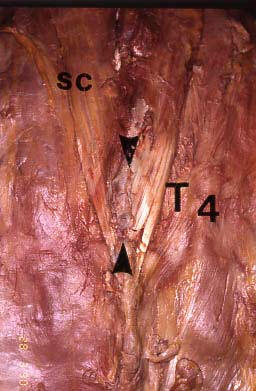
Three
Author's dissections. Left: a view of the
superficial exit of the cutaneous dorsal ramus of T4, through the superficial
layer of the rhomboideus (the fibers of which having being moved away) and,
deeper, through the tendon of the splenius cervicis, which attaches on the
lateral aspect of the spinous process of T4 and on the adjacent structures.
Middle: an entrapped cutaneous thoracic dorsal ramus (black arrows) after
having removed the thigh orifice. Left: another cutaneous dorsal ramus with
a mark of entrapment.
This
condition seems to be very rare, in contrast with an anatomic study showing
that entrapment is a common feature of the thoracic nerves (Maigne et al).
Muscular
sprain is a very common diagnosis, but there is no evidence to support it.
Travell
and Simons have developed the concept of myofascial pain and trigger points.
A trigger point is a very tender and hypersensitive spot within a muscle (or
in an aponeurosis, a tendon or even in the subcutaneous tissues), the pressure
of which reproduces the actual pain and its radiations. At the thoracic level,
these authors describe trigger points in muscles such as longissimus dorsalis,
iliocostalis, semispinalis, rhomboideus, levator scapula, etc... One of these
points is located in the multifidus, projecting over the vertebral body of
T5 and seems to us of special interest (see below). The causes for trigger
points are many, including trauma, poor postures, repetitive movements, etc.
The
treatment includes local injections of an anesthetic or a cold spray over
the muscles to treat, followed by stretching.
Some
trigger points according to Travell and Simons.
On the left, iliocostalis, pars
thoracis. On the right, multifidus. Due to its same location, close to the
spinous process of T4, this trigger point ressembles the interscapular point
described by R. Maigne and anatomically studied by the Author.
|
|
Pain
referred from the lower cervical spine |
| |
1-
Interscapular pain of cervical origin
Robert
Maigne described what he called “interscapular pain of cervical origin”, considered
by him as a very common cause of thoracic pain (Maigne, 1967). The syndrome
is made of thoracic and cervical signs.
Thoracic
signs. The pain is felt between the scapulae, and can be reproduced by a
firm pressure on a tender point projecting over the body of T5, located close
to the midline. This tender point was labelled “interscapular point”. It was
viewed by R. Maigne as the superficial exit of the T2 nerve (in accordance
to certain anatomic plates). It is accompanied by an area of cellulalgia (skin
and subcutaneous tissues hypersensitivity to pinch and roll test) located
on the same side and distributed in the territory of the upper thoracic cutaneous
rami (mainly the T2 nerve).
Interscapular pain of cervical origin, as desribed
by R. Maigne. The pain is experienced in
the interscapular area and is in fact refered from the lower cervical spine.
The familiar pain is reproduced by a pressure on the "interscapular point",
left or right to the projection of T5. In R. Maigne 's view, this syndrome
is the most common explanation for dorsal thoracic pain.
Cervical
signs. At the cervical level (mainly at C5-6), a segmental dysfunction is
present on the same side. When this dysfunction is not felt (or perceived)
by the patient, there is no cervical pain and the only complaint is thoracic
pain. But in many cases of common neck pain, there is also a radiation to
the interscapular area, by the same mechanism.
In
the author’s view, the dorsal pain is a referral from the cervical level.
His hypothesis for explaining this link between the lower cervical levels
and the interscapular point is that a segmental dysfunction at the lower cervical
levels can induce hypersensitivity in the medulla, spreading to the adjacent
inferior levels, as far as the T2 metamere. As there is no cutaneous dorsal
ramus from C6 to T1, the closest adjacent level to C6 is the T2 dorsal dermatome.
Maigne stressed that this link also appeared in case of acute cervical radiculopathy,
which was often preceded by interscapular pain.
As
a consequence, the treatment (mostly manual, but also by facet injection)
is directed to the cervical spine, and its efficacy (if so…) is considered
as the definite proof of the cervical origin of the pain.
2-
The “interscapular pain of cervical origin” revisited
Ten years ago, we
underwent a clinical and anatomic study on this topic. Fifty three consecutive
patients with thoracic pain were examined. Among them, 40 (75.5%) had their
familiar pain reproduced by the pressure on the interscapular point. It appeared
that the most acute pain was elicited by an oblique pressure directed toward
the lateral aspect of the tip of the spinous process of T4 (and not a PA pressure
toward the facet). A metallic marker was sticked on the skin and these patients
were X-rayed. The marks projected on the body of T5 in the majority of the cases
(and sometimes T6), which did correspond to the spinous process of T4 (or T5).
Thus appeared a relationship between this anatomic spot and the interscapular
point.
Left: palpation of
the interscapular point. The spine must
be flexed forward, to stretch the dorsal structures. The most teder spot is
easily located by an oblique pressure (toward the midline) on the lateral
aspect of a spinous process. A metallic mark shows this spinous process projecting
over the body of T5, thus belonging to T4 (right).
In
the same time, we dissected on 17 cadavers. It appeared obvious that the only
anatomic structure corresponding to this interscapular point was the lower
attachment of the muscle splenius cervicis. In the classic textbooks of anatomy,
this muscle is portrayed with a lower attachment on the spinous processes
of T2, T3, T4 and T5. We did not find this disposition. Rather, the muscle
inserted mainly on the spinous process of T4 and on the adjacent interspinous
ligaments of T3-4 and T4-5 for its upper and lower fibres. It was the only
structure actually corresponding to the clinical data. Furthermore, we found
that each cutaneous dorsal nerve ran from the intervertebral foramen to the
spinous process, parallel to the lamina, and exited superficially close to
the tip of the spinous process. In other words, the T4 nerve (and not the
T2 nerve) exited at the level of the T4 spinous process. Interestingly, many
of these nerves exited through tendons and appeared pinched by them. Thus,
the prerequisite for an entrapment (or at least, an irritation) neuropathy
were present.
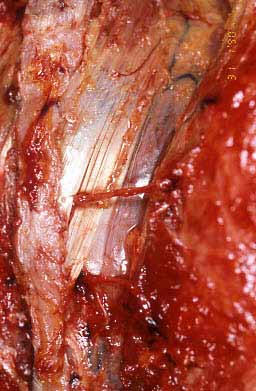
Samples
of our dissections (JYM).
Superior view, left: superficial layer of the upper back (trapezius removed)
showing the attachements of the splenius cervicis on the spinous process of
T4 (and, at a lesser extent, on the adjacent interspinous ligaments). Inferior
view, left: closer view of a left side (SC: splenius cervicis) with
two nerves (the cutaneous dorsal rami of T3 and T4) exiting through the tendon.
Superior view, right: another specimen, with dorsal rami appearing
through the tendon. Inferior view, right: right side, a nerve exits
through the tendon. See the
anatomic section for more details.
The
splenius cervicis is a thin superficial neck muscle, sharing its upper insertions
with the levator scapula on the transverse processes of the upper cervical
vertebrae. The two muscles belong to the same muscular layer. They run close
together along the spine, dividing to attach on the scapula laterally and
on the thoracic spine medially. The splenius syndrome resembles the levator
scapula syndrome. The causes could be a fatigue of the muscle, related to
prolonged neck postures, or to a dysfunction of the cervical spine.
A
facet origin has been advocated by Dreyfuss et al. By injecting a contrast
medium in the zygapophyseal joints of normal volunteers, they were able to
establish that these joints were a potential source of local and referred
pain under capsular distension. Evoked referral patterns were consistent in
all subjects. Significant overlap occurred in the referral patterns, with
most thoracic regions sharing 3-5 different joint referral zones.
R.
Maigne also described pain referred from the thoracic facet joints. In his
view, the pain followed the cutaneous dorsal ramus and was accompanied by
a stripe of cellulalgia within the dermatome.
Reprinted from R. Maigne:
distribution of pain arising from the thoracic facets. These areas also
correspond to areas of cellulalgia.
Cyriax
was the first to attribute thoracic pain to a slipped disc. For him, the pain
was dural for a part, elicited by the pressure of the protruded disc against
the thoracic dura mater. Some of the clinical features were a limitation in
thoracic flexion and the reproduction of the pain under neck flexion, coughing
or sneezing. He used to treat his patients by combining manipulation and traction.
Thoracic
MRI often reveals degenerated discs, or disc protrusion, but despite the lack
of studies addressing this topic, it can be assumed that, as at the lumbar
level, these abnormalities are frequent in asymptomatic subjects.

More
recently, thoracic discography has been used to investigate patients with
thoracic pain. A clinical concordance (reproduction of the familiar pain)
was found in approximately 50% of the cases. When the discogram was pathologic
(anular tears, intrinsic degeneration, and/or associated vertebral body endplate
infractions), this figure raised up to 75%. Control levels were usually painless.
Thoracic
pain has also been attributed to psychological factors. Some decades ago,
for example, the French Rheumatologic School considered it as exemplary of
a genuine psychological pain. The arguments were the lack of objective symptoms
(what practitioners of manual medicine, trained to spinal palpation, know
to be false), and the large female predominance (an insight into macho medicine!)
The
description of fibromyalgia has renewed this conception. The clinical features
of fibromyalgia resemble those of “psychogenic pain”. A neurologic mechanism
could be involved.
References